
Page 23 - ASCO Cultural Competency Toolkit
P. 23
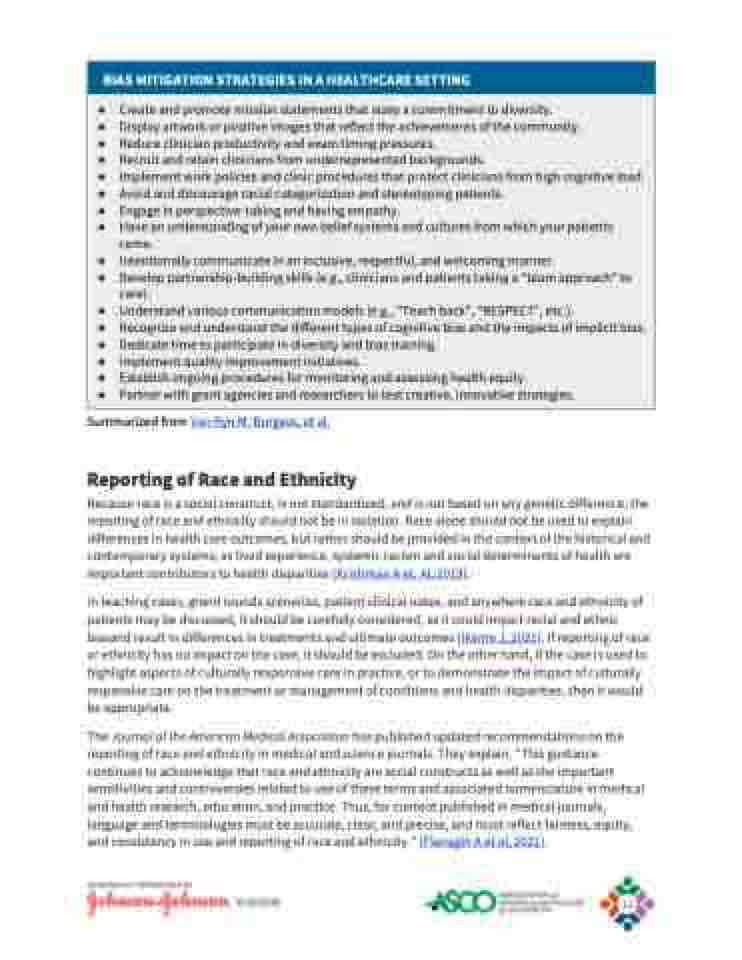
BIAS MITIGATION STRATEGIES IN A HEALTHCARE SETTING
● Create and promote mission statements that state a commitment to diversity.
● Display artwork or positive images that reflect the achievements of the community.
● Reduce clinician productivity and exam timing pressures.
● Recruit and retain clinicians from underrepresented backgrounds.
● Implement work policies and clinic procedures that protect clinicians from high cognitive load.
● Avoid and discourage racial categorization and stereotyping patients.
● Engage in perspective-taking and having empathy.
● Have an understanding of your own belief systems and cultures from which your patients
come.
● Intentionally communicate in an inclusive, respectful, and welcoming manner.
● Develop partnership-building skills (e.g., clinicians and patients taking a “team approach” to
care).
● Understand various communication models (e.g., “Teach back”, “RESPECT”, etc.).
● Recognize and understand the different types of cognitive bias and the impacts of implicit bias.
● Dedicate time to participate in diversity and bias training.
● Implement quality improvement initiatives.
● Establish ongoing procedures for monitoring and assessing health equity.
● Partner with grant agencies and researchers to test creative, innovative strategies.
Summarized from Van Ryn M, Burgess, et al.
Reporting of Race and Ethnicity
Because race is a social construct, is not standardized, and is not based on any genetic difference, the
reporting of race and ethnicity should not be in isolation. Race alone should not be used to explain
differences in health care outcomes, but rather should be provided in the context of the historical and
contemporary systems; as lived experience, systemic racism and social determinants of health are
important contributors to health disparities (Krishman A et. Al, 2019).
In teaching cases, grand rounds scenarios, patient clinical notes, and anywhere race and ethnicity of
patients may be discussed, it should be carefully considered, as it could impart racial and ethnic
biasand result in differences in treatments and ultimate outcomes (Ikeme J, 2021). If reporting of race
or ethnicity has no impact on the case, it should be excluded. On the other hand, if the case is used to
highlight aspects of culturally responsive care in practice, or to demonstrate the impact of culturally
responsive care on the treatment or management of conditions and health disparities, then it would
be appropriate.
The Journal of the American Medical Association has published updated recommendations on the
reporting of race and ethnicity in medical and science journals. They explain, “This guidance
continues to acknowledge that race and ethnicity are social constructs as well as the important
sensitivities and controversies related to use of these terms and associated nomenclature in medical
and health research, education, and practice. Thus, for content published in medical journals,
language and terminologies must be accurate, clear, and precise, and must reflect fairness, equity,
and consistency in use and reporting of race and ethnicity.” (Flanagin A et al, 2021).
GENEROUSLY SPONSORED BY
21
