Eye on Optometry
 Eye on Optometry recently asked students and graduates to tell us what they consider to be the Best Things about Optometry School. And while the answers convey a lot about optometry school, they say just as much about the students and graduates themselves. For starters, their enthusiasm for all things optometry school — and optometry in general — is obvious.
Eye on Optometry recently asked students and graduates to tell us what they consider to be the Best Things about Optometry School. And while the answers convey a lot about optometry school, they say just as much about the students and graduates themselves. For starters, their enthusiasm for all things optometry school — and optometry in general — is obvious.
First-year students tend to be very happy about the small class sizes they encounter at optometry school. As one of them notes, “I get to actually know people!” The whole atmosphere is invigorating, they say, “seeing how motivated everyone is and how hard everyone works and helps each other, all because we have the same ultimate goals.” They find it quite nice, too, “how everyone there finally understands your obsession with eyeballs.”
Speaking of getting to know classmates, one first-year student describes optometry school as an “inclusive community.” A third-year student puts it like this: “I had always heard that optometry is more like a family than a profession, but I just didn’t understand how that could happen. But after being here at school for only a few short weeks, I quickly saw my class turn from individual students into one big family. We are all so very supportive of each other not only in the classroom but in the clinic and also outside of school.” All through school, one 2015 graduate says, he liked “learning in a community setting where the entire class is rooting for me to pass my exams and proficiencies.” Graduates in particular use the word “lifelong” to describe their optometry school friends.
 Being totally engaged in their education and preparing for their career is a common attribute of optometry students regardless of what year they are. Every top list mentions some sort of relevant activity, including extracurriculars. Some examples: the opportunity to be part of many optometry organizations; traveling to other cities for conferences; making a difference through volunteering, political activism and social networking; “being involved in AOSA and establishing my roots in organized optometry.” As one first-year student sees it, “If you’re bored in optometry school, you’re doing it wrong.”
Being totally engaged in their education and preparing for their career is a common attribute of optometry students regardless of what year they are. Every top list mentions some sort of relevant activity, including extracurriculars. Some examples: the opportunity to be part of many optometry organizations; traveling to other cities for conferences; making a difference through volunteering, political activism and social networking; “being involved in AOSA and establishing my roots in organized optometry.” As one first-year student sees it, “If you’re bored in optometry school, you’re doing it wrong.”
 Optometry students’ and grads’ Best Things lists also show they genuinely enjoy what they do in optometry school and appreciate its value in preparing them for their careers. Even studying makes a few lists! From a third-year student: “Studying becomes much more fun in optometry school because it is all things that are interesting to you and something that you will actually be able to apply in clinic.” The lists reveal a love of learning optometry as well, with the Bests including learning about ocular diseases; fitting contact lenses; learning how to use the phoropter; “practicing techniques and watching how much you improve over the year”; learning something new about the eye every day; and finding the optic nerve for the first time. And when it’s time to work with patients in clinic, “completing the first full eye exam is one of the best feelings in the world.” Also a thrill: “Giving your patient their first pair of glasses/contact lenses and seeing their reaction.”
Optometry students’ and grads’ Best Things lists also show they genuinely enjoy what they do in optometry school and appreciate its value in preparing them for their careers. Even studying makes a few lists! From a third-year student: “Studying becomes much more fun in optometry school because it is all things that are interesting to you and something that you will actually be able to apply in clinic.” The lists reveal a love of learning optometry as well, with the Bests including learning about ocular diseases; fitting contact lenses; learning how to use the phoropter; “practicing techniques and watching how much you improve over the year”; learning something new about the eye every day; and finding the optic nerve for the first time. And when it’s time to work with patients in clinic, “completing the first full eye exam is one of the best feelings in the world.” Also a thrill: “Giving your patient their first pair of glasses/contact lenses and seeing their reaction.”
 Faculty are a fixture on the lists, from first-year students’ to graduates’. A graduate recalls “supportive faculty who devote all their energy towards making me a better doctor,” and a first-year student remembers realizing that “your professors are world renowned experts in their field.” A third-year student’s list includes “Faculty that are dedicated to helping you succeed.”
Faculty are a fixture on the lists, from first-year students’ to graduates’. A graduate recalls “supportive faculty who devote all their energy towards making me a better doctor,” and a first-year student remembers realizing that “your professors are world renowned experts in their field.” A third-year student’s list includes “Faculty that are dedicated to helping you succeed.”
 But there’s more to optometry school than, well, optometry school. A third-year student notes how he likes having “schedules that are busy but still allow time to have fun outside of school.” Formal and semi-formal “Eye Balls” that take place at many of the schools and colleges of optometry are a student favorite. Students also take advantage of the scene around them. You may guess where one graduate learned to perform a comprehensive eye exam in Spanish and took “study breaks on the beach,” (Puerto Rico), and, while it could be a lot of places, where a first-year student raves about “the food in the area!” (Berkeley, Calif.) Also appearing among the Best lists are the perks that come with optometry school, such as discounted or free eyecare publications; “being able to try every brand of contact lens so we can speak about them from experience”; attending national conferences at a discounted rate; and “being able to answer all the questions your family and friends have about their eyes.”
But there’s more to optometry school than, well, optometry school. A third-year student notes how he likes having “schedules that are busy but still allow time to have fun outside of school.” Formal and semi-formal “Eye Balls” that take place at many of the schools and colleges of optometry are a student favorite. Students also take advantage of the scene around them. You may guess where one graduate learned to perform a comprehensive eye exam in Spanish and took “study breaks on the beach,” (Puerto Rico), and, while it could be a lot of places, where a first-year student raves about “the food in the area!” (Berkeley, Calif.) Also appearing among the Best lists are the perks that come with optometry school, such as discounted or free eyecare publications; “being able to try every brand of contact lens so we can speak about them from experience”; attending national conferences at a discounted rate; and “being able to answer all the questions your family and friends have about their eyes.”
If we had to pick a sentiment that shined through from the stack of Best Things about Optometry School lists we received, it would be, as one student writes, “becoming someone who will make a difference in people’s lives.” And this list item from a first-year student kind of sums it all up: “I love optometry school because we’re all working our hardest to become doctors who will one day be able to really help people to see. The long hours, the hard exams, the gallons of caffeine will all be worth it, and in the meantime we’re all in this together.”

Eye on Optometry thanks the students and graduates who sent us their lists of Best Things about Optometry School: Keylee Clemons Brown, OD, 2015 graduate, Inter American University of Puerto Rico School of Optometry; Elizabeth Brubaker, third year, The Ohio State University College of Optometry; Mina Choi, first year, University of California – Berkeley School of Optometry; Amanda Himmel, first year, Michigan College of Optometry at Ferris State University; Emily Krueger, second year, Michigan College of Optometry at Ferris State University; Aaron Tai, third year, Illinois College of Optometry; Lawrence Yu, OD, 2015 graduate of Southern California College of Optometry at Marshall B. Ketchum University; and Ashley Zinser, fourth year, Northeastern State University Oklahoma College of Optometry.
One of the many appealing elements of a career in optometry is the variety of settings in which doctors of optometry can work. We asked ODs from several different practice types to answer some questions, including what they find most challenging and most rewarding about their job, to give you a glimpse into the possibilities. Part II of this blog will cover the following settings: large group private optometry practice, private practice (two owners), corporate optical adjacent and the opththalmic industry.
LARGE GROUP PRIVATE OPTOMETRY PRACTICE
 Antonio Chirumbolo, OD
Antonio Chirumbolo, OD
(State University of New York College of Optometry, Class of 2013)
Employed with Complete Family Vision Care, an eight-OD, multi-location group private practice in the Pittsburgh area
What does your practice setting have in common with other practice settings?
The setting in which you practice can differ dramatically, but that doesn’t necessarily have to dictate how you practice. Although I practice in a large group setting, I perform many of the same daily tasks as eyecare providers in other practice modalities.
In what ways does your practice setting differ from others?
Practicing in a large group setting can give you access to a very large patient base, which means that you have ample opportunity to see a diverse population of patients with different eye disease and conditions. It can also afford you the opportunity to practice to your full scope. It’s not uncommon for each doctor to have different strengths within the practice, from pediatrics to specialty contact lens fitting. This allows us to keep a lot of patients in-house rather than refer them out.
How is the bulk of your average work day spent?
The bulk of the day is spent seeing patients and billing and coding. Very little of my day is spent on practice management because we have dedicated staff and a dedicated owner handling the business aspect of the group.
What other tasks/roles are included in your work day?
I’m always working on ways to build the practice. Whether it’s scheduling local school screenings or developing various marketing materials such as newsletters and advertisements, there is always something to be done when I’m not seeing patients. Brainstorming and working with staff to develop practice-building opportunities is something we routinely work on.
What do you consider the biggest challenge of working in this setting?
Working in such a large practice and seeing so many patients can become overwhelming at times. It’s not uncommon for me to see more than 30 patients a day, and many of the cases are complex and involve special testing. Because we see a lot of pathology at our practice, it can be heartbreaking telling a patient they are suffering from a sight-threatening condition, or have suffered irrevocable damage to vision, which may or may not return.
What do you consider most rewarding about working in this setting?
A majority of the patients I see have been coming to see us for their eyecare needs for decades. Seeing the same patient year after year is very rewarding as you build intimate relationships with them and develop a strong rapport. These patients become extended family members. It’s also a great feeling to have a group of experienced doctors working with you. As a new(er) graduate, it’s not uncommon to run into cases or conditions that you might not be sure how to handle or manage. It’s always a good feeling when you can get the opinion of experienced doctors!
What is your work schedule?
I work six days a week, Monday through Saturday. However, we are only open every other Saturday from 8 a.m. to noon. Tuesday through Friday we work 9 a.m. to 5 p.m. Mondays we work from 9 a.m. to 8 p.m.
What aspect(s) of your practice setting might other doctors not like?
It can be difficult to build your practice within the practice, so to speak. That’s why it’s important to involve yourself in the community and get to know people. That takes a lot of hard work and energy and often takes time outside of the usual working hours. In other words, it involves a lot more than just seeing patients to be successful in this practice modality.
What advice would you give about choosing a practice setting?
Envision the type of days you want to have. If your goal is to punch a clock and check out at 5 p.m. every day, private practice is probably not going to be a good setting for you. It’s not uncommon for me to work after hours or call patients or pharmacies on the weekends. If you want to be part of something, and immerse yourself into building a practice, and stay somewhere long-term, then private practice is a great avenue. It’s also a great way to be your own boss in the sense that you have authority over what type of culture and experience for patients you want your practice to reflect.
PRIVATE PRACTICE, TWO OWNERS
 Thanh Mai, OD
Thanh Mai, OD
(Southern California College of Optometry at Marshall B. Ketchum University, class of 2012)
Co-owner of Insight Vision Center, Costa Mesa, Calif.
What does your practice setting have in common with other practice settings?
Every individual has different strengths, weaknesses, and a unique approach to patient care. Having a partnership allows for multiple viewpoints and more creativity in terms of offering the widest range of services to patients and in terms of building a practice.
In what ways does your practice setting differ from others?
We focus on vision therapy and specialty contact lenses. Because of this most of our patients are children, some very young, who we’re treating for conditions such as double vision or progressive myopia. Having a partner in practice to immediately consult with and bounce ideas off is a great benefit in treating patients with very challenging visual problems.
How is the bulk of your average work day spent?
Some days are devoted mainly to patient care. Some days we purposely see fewer patients in order to devote time to managing the practice.
What do you consider the biggest challenge of working in this setting?
We have a relatively new office so our biggest challenge is creating awareness of our unique services to potential patients in our area.
What do you consider most rewarding about working in this setting?
The ability to create a culture that really appreciates patients and treats them as close friends and family.
What is it like working with children compared to with adults?
I could write books about this! Children are such a mixed bag and each one has such a different personality that evolves in the short amount of time you see them. One aspect I like about working with children is being able to create a change that can positively affect them for the rest of their lives. It’s quite exciting.
What advice would you give about choosing a practice setting?
Don’t just look for a job. Begin your career thinking about why you wanted to become an optometrist in the first place. Practice in the area you want to live, where you find the most happiness and fulfillment vs. choosing your location based only on your career opportunities.
CORPORATE OPTICAL ADJACENT
 Nikil Patel, OD
Nikil Patel, OD
(Indiana University School of Optometry, class of 2004)
Owner of practice (Vani Vision) leasing space from Costco in Atlanta, Ga.
What does your practice setting have in common with other practice settings?
The eye exam area is similar to other practice settings. We have two fully equipped exam lanes, including digital refraction systems. We have a pre-test area that includes an autorefractor, non-contact tonometer, wide-field retinal imaging, and a corneal topographer. (I own some of the equipment, and Costco provides some equipment.) Like other practice settings, we have many diagnostic contact lenses.
In what ways does your practice setting differ from others?
The main difference is we don’t have a dispensary and thus don’t sell contact lenses or eyeglasses. (Costco does.) I’m able to concentrate my efforts only on optometry and not on retail and merchandising, which are different skills.
How is the bulk of your average work day spent?
The bulk of my day is examining patients. I have a very large medical practice that continues to grow and takes the majority of my schedule.
What other tasks/roles are included in your work day?
I have managerial tasks such as paying bills, overlooking financials, managing two employees. I also keep up with the industry and constantly read about all aspects of optometry.
What do you consider the biggest challenge of working in this setting?
The biggest challenge is not having control of the actual building and thus not being able to set my own hours. I can only be open when Costco is open. It’s likely similar to other offices where a landlord or a partnership is involved. Both parties need to be considered.
What do you consider most rewarding about working in this setting?
Most rewarding about this setting is that patients appreciate that there is no financial bias in my recommendations for eyeglasses or contact lenses. I’m not selling them anything, and I believe because of that they tend to adhere to my recommendations.
What is your work schedule?
I work Monday through Thursday 10 a.m. to 6 p.m., and Fridays 10 a.m. to 5 p.m., with a one-hour lunch each day. I’m off Saturday and Sunday.
What aspect(s) of your practice setting might other doctors not like?
Most optometrists make the largest portion of their revenue on eyeglasses or contact lens sales. Working in a corporate-affiliated environment means your practice revenue is solely derived from the patient care interaction, so embracing a medical practice is almost a necessity to grow.
What advice would you give about choosing a practice setting?
Be open-minded and try out different settings. The best way to see which modality is best for you is to work in each for a period of time. Coming out of school, there are many opportunities for hours within different practices, which can be a great guide for your long-term career.
OPHTHALMIC INDUSTRY
 Mohinder Merchea, OD, PhD, MBA
Mohinder Merchea, OD, PhD, MBA
(The Ohio State University College of Optometry, class of 1997)
Employed by Alcon in Fort Worth, Texas, as Head of Medical Affairs for Vision Care in the U.S. and Canada
What are the key characteristics of your practice/employment setting?
Medical Affairs at Alcon provides scientific support for late-stage product development and post-market support for medical devices and drugs in the form of clinical trials, medical publications, training and education. Medical Affairs is located within the Alcon corporate headquarters along with other business functions such as Research & Development, Legal, Regulatory and Commercial.
In what ways does your setting differ from others?
A Medical Affairs role in industry doesn’t typically involve direct patient care, but we do have clinical facilities to provide demonstrations or training to eyecare practitioners on the products within Alcon’s portfolio in Vision Care and Surgical.
How is the bulk of your average work day spent?
The majority of my day is spent working with people from all areas of the business to ensure that eyecare practitioners understand how Alcon’s products can help patients see, look and feel their best.
What other tasks/roles are included in your work day?
Medical Affairs helps to formulate publications and presentations at scientific meetings and through journal articles. Medical Affairs also provides the scientific input and expertise in the design or review of marketing materials and tools. We communicate with and support external experts and opinion leaders. We also help respond to questions from patients about our company’s products, and serve as disease state experts to answer questions from internal colleagues.
What do you consider the biggest challenge of working in this setting?
I miss the feeling of successfully fitting a post-surgical cornea or late-stage keratoconus patient and seeing their faces light up with joy when they regain the gift of vision. In industry, that satisfaction of helping patients is indirect but no less satisfying when an eyecare practitioner tells you their patient is wearing a contact lens that you helped design.
What do you consider most rewarding about working in this setting?
In Medical Affairs, I get to represent the voice of the eyecare professional and patient within my business. The decisions or recommendations we make related to a medical device or drug have the opportunity to help millions of patients, so it’s amazing to think about that from a public health significance standpoint.
What is your work schedule?
There’s no such thing as a 40-hour work week, but it really comes down to your individual motivation and drive. In my current role, I have responsibility for the United States and Canada, so the majority of my work is during the day. Prior global roles required late-night conference calls working with colleagues from around the world.
What aspect(s) of your practice setting might other doctors not like?
In my role, what I am working on changes day to day, or faster in some cases. If you’re a person who loves routine, industry in general and medical affairs could be frustrating. If you thrive in dynamically changing environments, if you’re comfortable making decisions efficiently, and you like to learn constantly, medical affairs can offer you a fulfilling career path.
What advice would you give about choosing a practice setting?
Optometrists have a wide variety of career paths they can take in addition to clinical practice. The best advice is talk to your peers and visit the settings you think you’re interested in for a day to see if they excite you.
One of the many appealing elements of a career in optometry is the variety of settings in which doctors of optometry can work. We asked ODs from several different practice types to answer some questions to give you a glimpse into the possibilities. Part I of this blog will cover the following settings: academic practice, solo private practice, U.S. Department of Veterans Affairs and corporate. Other practice settings will be covered in Part II.
ACADEMIC PRACTICE
 Valerie Kattouf, OD, FAAO
Valerie Kattouf, OD, FAAO
(Illinois College of Optometry, class of 1995)
Associate Professor and Chief of the Pediatrics and Binocular Vision Service at Illinois College of Optometry and Clinical Instructor at the University of Chicago
What does your practice setting have in common with other practice settings?
We are very high volume and, just like most practices, we serve patients of all ages. We see routine refractive errors, fit contact lenses, and treat infants, toddlers, school age children, and adults with a range of visual needs. I see a number of adult patients with double vision issues because our practice encompasses binocular vision care.
In what ways does your practice setting differ from others?
The majority of our patient encounters are complex, involving issues such as complex refractive error, pathology, systemic syndromes, amblyopia and strabismus, so we perform less routine care. Also, our patient population is primarily Medicaid. We do accept private insurance plans, but the majority of our population is underserved. We also work with students, teaching while administering patient care, which is a different way of approaching things.
How is the bulk of your average work day spent?
This is a difficult question to answer for the academic setting because of the variety of roles we have. Some days are primarily clinic, while some days are spent working on administrative issues. I spend a good deal of time preparing lectures for classroom teaching as well as giving continuing education courses around the country. It is this constant variety that makes my career challenging and exciting.
What other tasks/roles are included in your work day?
Administrative tasks, continuing education and seminar lecture preparation, classroom teaching, clinical teaching, research activity, medical record completion, and student clinical evaluations.
What do you consider the biggest challenge of working in this setting?
The patient volume, complex care in clinic, and juggling the other responsibilities. Sometimes the days feel too short.
What do you consider most rewarding about working in this setting?
Helping patients who may not always be able to help themselves. I also enjoy when graduates let me know that I helped them to feel more confident in their abilities, which is always my goal when teaching.
How does having children in the patient mix differ from seeing all adults?
There’s never a dull moment. Pediatric care is fun, but you have to be adaptable and willing to vary from the norm. It’s a true honor to be able to guide parents to the proper treatments for their children and help them to understand the impact of the treatments on all aspects of the child’s life.
What is your work schedule?
I work five days per week, Monday through Friday. My hours vary. I suppose my on-campus hours are 40 per week. I do bring a great deal of work home to do at night, particularly things that I don’t want to dominate my time on campus, such as completing lectures, student evaluations, and medical records.
What advice would you give about choosing a practice setting?
If you can never feel like you have a job, but instead that you’re investing in your career, you’ll never feel like you’re working. My workplace environment is an extension of my family. I love being there, I adore my colleagues, and I feel honored to see patients and teach students daily. Find an environment that inspires and challenges you daily where you feel warmth and purpose.
SOLO PRIVATE PRACTICE
 David Hite, OD
David Hite, OD
(Southern College of Optometry, class of 2013)
Owner of North Range Eye Care in Commerce City, Colo.
What does your practice setting have in common with other practice settings?
Routine patient care is virtually the same wherever you practice. The difference may be in who makes decisions about office flow and how much time you spend with patients.
In what ways does your practice setting differ from others?
I started the practice cold, and in less than three years we have all the technology we need to manage the full eyecare spectrum. As a private practice owner, I have full control of my schedule, how I see patients, and the overall patient experience.
How is the bulk of your average work day spent?
Patient care takes up the majority of my time in the office.
What other tasks/roles are included in your work day?
As the owner of a private practice, patient care is not all I do. In addition to patient care, I take care of overseeing the various departments of the practice, doing payroll and accounting, and taking care of small office maintenance items as well. My wife works in the office, too, and our first child, Dawson, came to work with us every day until he was a year and a half old.
What do you consider most rewarding about working in this setting?
There is a different feeling in seeing patients when you are the owner. You care more about their experience and their final outcome. There is more reward when they have a good experience. Having patients refer family or friends becomes a very personal recommendation for you.
What is your work schedule?
We see patients five days a week, but two days a week we don’t see patients in the mornings. That time is either my time off or time to work on administrative tasks. We don’t work weekends or late hours.
What advice would you give about choosing a practice setting?
Wherever you work, you’ll be building someone’s dream. That could be the owner of a private practice if you are an employee, a corporation, or your own personal practice. If you’re working hard, make sure you’re the one benefiting in the end.
U.S. DEPARTMENT OF VETERANS AFFAIRS
 Laura Dowd, OD, FAAO
Laura Dowd, OD, FAAO
(New England College of Optometry, class of 2009)
Staff Optometrist and Optometry Student Program Coordinator in the VA Maine health system
What does your practice setting have in common with other practice settings?
We see patients with a wide variety of eye conditions. We prescribe glasses, treat eye diseases and co-manage surgical patients like many other practices.
In what ways does your practice setting differ from others?
The VA setting is an adults-only patient population, and the patient base is generally older males. The VA also has a universal electronic medical record that contains each patient’s entire health record and is able to link to other VA hospitals. The VA also has resources that practices may not, such as low vision and blind rehabilitation services. The eye clinic is part of the patient’s whole healthcare team, not just an individual service.
How is the bulk of your average work day spent?
A majority of my day is spent seeing patients or precepting students.
What other tasks/roles are included in your work day?
Most days include a didactic activity or group meeting, such as optometry journal club, interprofessional education, grand rounds or staff meetings. I also have administrative duties, including triaging consults and coordinating student schedules with the education office.
What do you consider the biggest challenge of working in this setting?
The VA is a large organization with many regulations and layers. I have a certain amount of control within the eye clinic but little to no control over IT, HR, contracting, etc.
What do you consider most rewarding about working in this setting?
Taking care of veterans and having ample time to teach.
How does the VA patient population differ from others and how does that affect your job?
The VA population tends to be elderly, and a majority of patients are male. While most practices draw from a small area, my VA encompasses a large geographic area. Significant travel distances and transportation issues, in addition to caring for the elderly patient, require extra consideration to maximize patient care. For example, it may not be practical to have a patient return next week for a visual field test if he lives three hours away and the shuttle van only goes to his region one day a week. This often leads to squeezing in extra testing that day or overbooking my schedule to “piggyback” my appointment onto a day when the patient is already scheduled for a different specialty visit at the VA. It takes a certain amount of strategizing to effectively and appropriately treat the patient in the most efficient manner.
What is your work schedule?
I work 40 hours a week (four 10-hour days with Fridays off). I do not have any nights or weekends at the VA.
What advice would you give about choosing a practice setting?
Optometry students should expose themselves through their training to a variety of practice modes. When they’re ready to graduate, they can lean on these experiences. They should also remember that their first job will not likely be the perfect job and they don’t have to stay in the mode for the rest of their career.
CORPORATE OPTICAL ADJACENT
Abby Hsu, OD
(Western University of Health Sciences College of Optometry, class of 2013)
Employed as Managing Optometrist by EYEXAM, next to LensCrafters, in Montclair, Calif.
What does your practice setting have in common with other practice settings?
Quality eye care and professionalism. We put the patient first.
In what ways does your practice setting differ from others?
Most eyeglass prescriptions are available within one hour, and a wide variety of contact lenses are available.
How is the bulk of your average work day spent?
Seeing patients, managing the business, overseeing staff, partnering with the LensCrafters general manager to improve the business.
What other tasks/roles are included in your work day?
Training the staff, ordering and re-stocking contact lenses.
What do you consider most rewarding about working in this setting?
The wide variety of patients I see and establishing a relationship with them year after year. The wide variety of frames and contact lenses and the access to advanced technology.
What is your work schedule?
I work 40 hours/week, usually Tuesday through Saturday. In the retail setting, we’re open seven days a week. Another doctor works on the two days I’m off.
What advice would you give about choosing a practice setting?
Find your niche based on factors like practice speed and patient demographics. If you have an interest in low vision, vision therapy or contact lenses, find a practice that focuses on that.
Technology is an integral part of practicing medicine today, and optometry is no exception. Diagnostic technologies in particular have advanced rapidly. As the latest instruments make their way into clinical practice, they also become part of optometric education. The schools and colleges of optometry are committed to ensuring their students graduate with a full understanding of state-of-the-art technology. Many of the diagnostic technologies that optometry students are using today are game-changers for patient care.
► Optical coherence tomography (OCT) is one example. Today’s widely used OCT instruments allow the capture of cross-sectional images of ocular tissue structure with resolution as high as 3 microns.
 |
| OCT imaging of bullous keratopathy with a bandage contact lens |
That’s a really close look when you consider that a micron is one-millionth of a meter. One inch contains about 25,000 microns, and the eye of a needle contains about 1,200 microns.
OCT has replaced more invasive diagnostic tests as the primary way of monitoring the progression of many retinal conditions and diseases and their response to treatment. OCT also provides high-resolution visualization of anterior segment structures such as the cornea and angle, and measures the thickness of the retinal nerve fiber layer to aid in the diagnosis and monitoring of glaucoma and other diseases of the optic nerve. Anterior segment
 |
| Anterior segment OCT of a scleral contact lens on the eye |
OCT is also used to custom design specialty contact lenses and evaluate proper fit. Originally adopted by specialists, “OCT has become an essential component of primary eye care,” says Thomas A. Wong, OD, Director of New Technologies at SUNY State College of Optometry.
 |
| Thomas A. Wong, OD, Director of New Technologies at SUNY State College of Optometry, and fourth-year student Elizabeth Usupov with a refractive power/corneal analyzer that is part of SUNY Optometry’s “Digital Eyecare Practice of Tomorrow.” |
Most recently, new software algorithms have allowed OCT instruments to perform angiography as well. OCT angiography enables a three-dimensional view of separate layers of retinal blood vessels, including deeper layers not clearly seen with other forms of angiography — without the need to inject dye into the patient’s arm. Its speed and non-invasiveness could revolutionize how and by whom angiography is utilized.
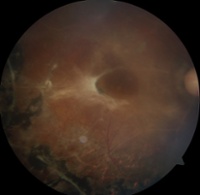
 |
| Normal retina as viewed with widefield imaging |
► Traditional fundus photography, while essential for documenting retinal findings from a comprehensive exam, can only capture images of the posterior pole, i.e., about 45 degrees of the back of the eye. Widefield retinal imaging, however, uses scanning lasers to produce images representing up to 200 degrees. Therefore, it enables detection of pathology in the peripheral retina that would not be detected with traditional retinal photography or slit lamp exam. A growing body of research shows that many retinal disease processes manifest first in the periphery.
 |
| Fundus photography of proliferative diabetic retinopathy |
Some widefield retinal imaging devices also have fundus autofluorescence (FAF) capability. FAF is another exciting new technology, which non-invasively detects certain byproducts of retinal metabolism that are believed to indicate high risk for disease development. The byproducts, called fluorophores, illuminate, i.e., fluoresce, when exposed to a particular wavelength of light.
 |
| Fundus photography of non-proliferative diabetic retinopathy |
► Dry eye, one of the most common ocular conditions, has been difficult to diagnose and manage due to multiple causes and signs and symptoms that vary among patients and overlap with other forms of ocular surface disease. Things got a lot more definitive, however, with the introduction of tear osmolarity testing. Elevated tear osmolarity is a hallmark of dry eye disease and can be used as a metric for diagnosing and determining the severity of dry eye. Tear osmolarity can now be tested in-office quickly and easily, giving doctors an objective and reliable way to diagnose dry eye and monitor treatment. It’s possible, too, for a patient to have ocular surface damage from dry eye but no symptoms, another reason objective testing is such a huge and important paradigm shift.
 |
| Fundus autoflourescense of a normal eye with multiple water droplet artifacts |
Other dry eye-related innovations are imaging of the tear film and the meibomian glands using interferometry/topography devices. The new diagnostic tools that utilize these strategies enable objective analysis of the tear film that protects the ocular surface. They measure the actual thickness of the lipid layer of the tear film and provide a much better view of the meibomian glands than can be achieved with the naked eye. Armed with this information, optometrists can better distinguish between two main types of dry eye (aqueous deficient, i.e., reduced tear production, and evaporative, which is gland- and lipid layer-related) and prescribe the appropriate treatment. “For too long we have not had a truly systematic, scientific approach to many common conditions like dry eye. Patients have often been treated in a random fashion. These technologies are leading us to more personalized therapies, which is a growing trend in medicine,” Dr. Wong notes.
 |
| Meibomian gland imaging |
 |
| Spectral microscopy analysis, count and health of corneal endothelial cells |
► Specular microscopy is an imaging technology for evaluating the corneal endothelium, which is responsible for nourishing and keeping the cornea transparent. Humans are born with a fixed number of corneal endothelial cells, so preserving their numbers and health is crucial for sight. Specular microscopy can not only count the number of endothelial cells but also reveal their size, shape and density, all of which can be negatively affected by disease as well as contact lens overwear. This technology enables earlier and more accurate diagnosis of these problems because such detailed and objective information isn’t obtainable by clinical exam alone.
► Even optometry’s oldest undertaking, refraction, is evolving with advances in technology. Today, refractions can be performed with automated digital equipment, rather than manually, and therefore can be instantly optimized with diagnostic imaging tools and wavefront aberrometry. (Wavefront aberrometry was first developed by astronomers attempting to improve their view of objects in outer space.) With these state-of-the-art refractions, information about how key structures along the optical pathway are affecting vision can be obtained. A wealth of objective data is utilized, which greatly improves accuracy and efficiency compared with standard refractions. The days of seemingly endless “which is better, number one or number two?” may be numbered. The new refractions also help determine the best possible prescription for a patient’s needs, which, for example, may be different for the office, playing sports or driving at night. Digital refractions based on this added data are helping primary care optometrists to provide the best possible vision for patients. They’re also paving the way to the goal of thefuture: the ability to make glasses and contact lenses to ultra-precise specifications that match the precision of the refraction and provide patients with true “high-definition vision.”
 |
| Multiple data sets from the optical pathway captured by one instrument to be used as part of a digital refraction |
In a nutshell, “The technologies available to our interns assist them tremendously in understanding how the eye functions and what structural changes occur in the presence of a disease state,” says Robert L. Gordon, OD, FAAO, DPNAP, Clinical Director and Associate Dean of Clinical Affairs at the Western University of Health Sciences College of Optometry. “They provide a window for looking at the various layers of the eye’s structure that lie beneath the surface tissues seen by direct observation.” And a window to their future as optometrists, too. Lorie Lippiatt, OD, President of Salem Eyecare Center in Ohio, a practice that makes it a point to stay on the cutting edge, puts it all in a broad context, saying “Technology vastly increases our diagnostic capabilities, allows us to take care of our patients in a streamlined fashion, and advances optometry in the medical community because we can obtain and communicate meaningful findings to a patient’s other healthcare providers.”
 |
| Lorie Lippiatt, OD, uses a digital refraction system at her Ohio practice |
 We are well in the New Year and I wish you a wonderful 2016.
We are well in the New Year and I wish you a wonderful 2016.
As I reflect back on 2015, there is much I would like to share.
I began my tenure as ASCO’s Executive Director this summer after long-standing Executive Director Marty Wall retired. The welcome I received has been so overwhelmingly positive and supportive – I greatly appreciate everyone making me feel at home so quickly. So far, the work has been challenging and extremely fulfilling.
Around the same time as I joined ASCO, Dr. David Heath, President of the SUNY College of Optometry, was elected ASCO President. Together, Dr. Heath and I are off to a good start. Of particular note, ASCO is embarking on a comprehensive strategic planning process to develop a five-year, organization-wide plan that will drive priority initiatives, annual work plans and budgets for the Association. The process will be as inclusive as possible and will include input from ASCO committees, special interest groups, staff and other stakeholders. Our goal is to have a finalized plan before spring 2017.
Highlights of 2015 include:
- The University of Pikeville, Kentucky College of Optometry became ASCO’s 22nd
- A special category of membership was developed for developing schools.
- Our first Online Clinical Educators Forum was held by ASCO’s Clinical Affairs Committee.
- ASCO held its first joint ASCO-American Academy of Optometry workshop “Charting Your Career in Academic Optometry.”
- ASCO received very generous support from a growing set of Corporate Contributors as well as sponsors for individual programs. We welcomed National Vision, Optos, Optovue, Safilo, and Vital Source Technology as new Corporate Contributors.
- We experienced a 5% increase in the number of optometry school applicants in the application cycle for 2014-2015 as compared to the previous cycle.
Some interesting stats from the Profile of the Entering Class (2014-2015 academic year) are:
- At the schools and colleges of optometry in the 50 states and Puerto Rico, there were a total of 6,805 optometry students enrolled during the 2014-2015 academic year
- 66.1% of the student body was female and 33.9% was male.
- The student body was 55.7% White, 29.1% Asian, 5.1% Hispanic or Latino, 3.1% African American, 0.6% American Indian or Alaskan Native, 0.4% Pacific Islander or Native Hawaiian, and 5.9% Other.
- The average GPA of the 2015 entering class was 3.43; and first year tuition and fees range from $17,556 to $55,184.
- The Joint Project on Further Developing a Robust, Diverse, and Highly Qualified National Applicant Pool continued promoting the profession in the following ways: virtual fairs, email campaigns, direct mail campaigns, search engine optimization, increased social media presence, videos, blogs,podcasts, publications (True Stories booklet and the revised Optometry Career Guide) and the completely revamped Inspiring Future ODs Program.
- ORMatch experienced a 3% increase in applicants in 2015 compared to the previous match cycle. Seventy-three percent of the residency applicants were matched and 86% of the available positions were filled. There were 210 residency sites with 411 available positions participating.
- The new platform for the Residency Directory opened in December.
- The Annual Faculty Data Report, containing 15 tables of data on faculty demographics, was released in March.
- The Annual Student Data Report, containing 43 tables of data on student enrollment, graduation figures and financial aid, came out in April.
- Dr. Glenn Hammack, Founding President, NuPhysicia LLC, received the first Dr. Lester Caplan honorary award lecture during the ASCO Clinic Directors SIG meeting in October.
- Plans were finalized for our inaugural Summit on Interprofessional Education and Practice, scheduled for early February.
- ASCO held a special joint board meeting with the National Board of Examiners in Optometry to discuss collaborative strategies for addressing current and future issues.
- The ASCO Public Health Educators SIG began working on the “Essential Public Health and Environmental Optometry Curriculum Content for Schools and Colleges of Optometry” document, which is modeled after our “Attributes of Students Graduating from Schools and Colleges of Optometry” document.
- James Sheedy, who was instrumental in forming the ASCO Ophthalmic Optics Educators SIG in 1996, was honored for his contributions in ophthalmic optics and delivered the Joe Bruneni Honorary Award Lecture entitled “Blue Light-Good or Bad?” in memory of Dr. Daryl Meister.
- The 6th Summer Institute for Faculty Development was held in July, supported by Alcon, Vistakon, Essilor, National Board of Optometry, Luxottica, Allergan, and the Partnership Endowment. 100% of this year’s program participants rated the sessions favorably. A few testimonials are:
“This was an overwhelmingly wonderful experience. I feel very fortunate to have been able to attend this training and will recommend to all my colleagues!”
“Very beneficial and wonderful institute! These sessions and lectures have been incredibly valuable as I develop my career. The speakers were very helpful and knowledgeable with their material. Thank you to everyone who coordinated and prepared this conference!”
“Excellent program provide[d] rejuvenation and passion for what I do.”
- The 3rd Future Faculty Program, supported by a generous contribution from Walmart, was also held in July, and 100% of this year’s program participants rated the sessions favorably as well.
- The ASCO Curriculum Guidelines for Culturally Competent Eye and Vision Care Workshop Grant Program held five cultural competency diversity workshops in 2015. Generously funded by Walmart, the program provides funds to schools and colleges of optometry for on-site Cultural Competency Curriculum Guidelines Implementation Workshops. The workshops demonstrate how to use ASCO’s guidelines to incorporate topics and experiences in cultural competency into the optometric curriculum. Workshops were held at: Michigan College of Optometry at Ferris State University (Jan); Southern College of Optometry (Feb); Midwestern University – Arizona College of Optometry (March); University of Alabama at Birmingham School of Optometry (March); and University of California – Berkeley School of Optometry (May).
- ASCO’s Journal, Optometric Education, was redesigned and emerged as a more technologically advanced and user-friendly publication with its Summer 2015 issue in July.
The journal appears online in a new format, equipped with new digital capabilities that make its content more easily searchable via Google Scholar and other search engines. All content is available as a web page, eliminating the need to open or download a PDF file. The redesign simplifies the finding and sharing of information for students and practitioners and improves the reading experience on all devices, including smartphones and tablets.
The updates also give ASCO corporate contributors and other supporters a new way to direct readers to their websites via a simple click-through. In addition, the new format and capabilities open opportunities for future discussions and forums online.
- Two additional podcasts were added to our podcast series in 2015: Optometry and Interprofessional Education and ASCO and New Beginnings.
- ASCO’s Awards Program was supported by International Vision Expo and Oculus.
- ASCO held almost 40 various meetings for committees, SIGs and other groups.
- Dr. Michelle Hoff, UCB, was our first non-corporate contributor with a very generous private contribution to the ASCO Ophthalmic Optics Educators SIG.
- We made infrastructure investments in new web-based applications and technology dealing with ASCO’s membership database, on-going operational surveys, centralized application system, centralized admission exam, residency match service, website and social media landing pages, etc.
- We presented Resolutions reflecting the Board’s appreciation to Dr. Roger Boltz (upon his departure from the Board ), Dr. Jennifer Coyle (for having served two terms as ASCO President), Dr. Earl Smith (for his induction into the National Optometry Hall of Fame), and Marty Wall (for his 24 years of service as ASCO’s Executive Director).
- ASCO Board members and staff represented optometric education at important industry meetings with the AAO, ABO, ACOE, AOA, ARBO, COPE, FASHP, NAEVR/AEVR, NAAHP, NBEO, IOM/NAM Global Forum, etc.
I am very encouraged by the work that we have completed and look ahead with optimism at the work that is to be done.
A very special thank you to all of our Corporate Contributors and sponsors. Your generosity has allowed ASCO to continue our vital programs that support optometric education.
Wishing you all a very bright 2016!
Sincerely,
Dawn Mancuso, MAM, CAE, FASAE
ASCO Executive Director
The curriculum for any student entering optometry school today will in some way include interprofessional education (IPE). IPE is a hot topic throughout medicine and an area of much activity in optometry. The Association of Schools and Colleges of Optometry (ASCO) is a leader in working to ensure optometry students are prepared to participate in interprofessional care (IPC) when they graduate. The Association’s “Attributes of Students Graduating from Schools and Colleges of Optometry” calls for recipients of the Doctor of Optometry degree to have the ability to appropriately use all resources, including ancillary personnel, intra- and interprofessional collaboration, co-management and referral, in ensuring the best quality of patient care and to be committed to working as an integral member of the larger interprofessional healthcare team to improve patient care outcomes.
Carole Timpone, OD, Distinguished University Professor and Associate Dean of Clinical Programs at Pacific University College of Optometry (PUCO), and Jennifer Coyle, OD, MS, PUCO Professor and Dean, and Chair of ASCO’s Interprofessional Education and Collaborative Practice Committee, explain the importance of IPE and IPC: “The demographics and needs of patients have changed dramatically. Chronic disease, which has a major impact on quality of life, has replaced acute illnesses as the leading burden to the healthcare system, including cause of death. Addressing these new needs and achieving the best outcomes requires a more comprehensive and ongoing approach to care with a focus on prevention. This is best delivered by a team of providers.”
Optometry Plays a Key Role
Optometry schools and the future optometrists they’re training have a distinct responsibility in building interprofessionalism. “Eye health and vision are significantly impacted by chronic diseases,” says Dr. Timpone. “The Doctor of Optometry is an integral member of the healthcare team in all aspects of care, from initial diagnosis and treatment to ongoing management, with the goal of ultimately improving or maintaining quality of life.” Melissa A. Vitek, OD, FAAO, Director of International and Continuing Education at Salus University Pennsylvania College of Optometry (Salus/PCO) and member of ASCO’s Interprofessional Education and Collaborative Practice Committee, elaborates, “Due to the fact that vision is so critical for even a basic level of functioning, an optometrist’s office is the point of entry into the healthcare system for many patients. To fully meet the needs of patients, optometrists need to be positioned to communicate effectively and efficiently with members of several different healthcare professions.”
Every school and college of optometry that’s a member of ASCO is currently engaged in some form of IPE. According to Dr. Timpone, the experiences range from sharing core courses with students from other health professions to integrated clinics that provide true team-based care. Many programs include interactive interprofessional case conferences, some beginning as early as the first year. For example, PUCO currently offers an elective course in interprofessional care for third-year students that blends face-to-face and online instruction with a clinical practicum. To complement IPE coursework, the University runs the Interprofessional Diabetes Clinic (IDC), which helps low-income, under-insured individuals manage their diabetes by bringing together healthcare providers from across the professions to provide care. Students, staff and faculty from PUCO, with other Pacific University health professions, including occupational and physical therapy, mental health, dental health science, physician assistants and pharmacy work in the IDC one Saturday each month. In addition, says Dr. Timpone, “We are developing an ‘IP Concentration’ recognition for students who have pursued IPE and IPC beyond the basic curriculum.”
Salus/PCO has a long history of interdisciplinary thinking, beginning in the 1970s in the field of low vision rehabilitation. Today, more than 300 students from the optometry, physician assistant, occupational therapy and speech language pathology programs are enrolled in the “Evidence-Based Practice: An Interprofessional Team-Based Approach” course, which is a requirement for first-year students. Salus/PCO students also participate in several interprofessional practice initiatives, which include a collaboration with a nursing school. Two interprofessional pilot programs, one involving the Veterans Administration and another involving clinical problem-solving via patient cases, are ongoing projects.
At Southern California College of Optometry at Marshall B. Ketchum University (SCCOMBKU), first-year students take Professional Ethics and Population and Public Health courses with physician assistant (PA) students. In their third year, they participate with PA students in interprofessional case conferencing in each of three quarters, notes Raymond H. Chu, OD, MS, Associate Dean for Academic Affairs. During the first session, the students get to know one another and address common misconceptions about their respective professions. In subsequent sessions, they tackle cases involving issues such as smoking cessation, diabetes and cultural competence. “The overarching objective with the IPE curriculum is to develop the primer in which students and eventually professionals have the comfort and ability to communicate with one another in an effort to support wellness and coordination of care,” Dr. Chu says.
Dr. Timpone points out that evidence of the benefits of IPE and IPC is beginning to appear in the professional literature. Studies are showing that IPE provided during the training of the healthcare workforce enables effective collaboration among professionals once they’re practicing and that the competencies they develop translate into improved health and patient care outcomes. Ongoing work in the area of IPE includes further development of curricula and assessment of effectiveness. The upcoming ASCO Interprofessional Education and Collaborative Practice Summit (Feb. 5-6, 2016, in Fullerton, Calif.) will assist in charting a course for the future.
Listen to Optometry and IPE podcast here.
What Optometry Students and Residents are Saying about Interprofessional Education and Care
Warren Morton, a first-year student at SCCOMBKU and President of the Class of 2019, says “It’s easy to see how important concepts from IPE can be in the real world when ultimately the patients have the most to gain from a more complete healthcare team.” Warren says it’s been interesting to see via the IPE curriculum how valuable PAs are for the country’s healthcare system and how OD and PA students approach ideas differently. He also says he’s realized that “failure to recognize the importance of working with other professions will leave our own profession at a disadvantage.” Because of her exposure to IPC at PUCO, Alexandra Bavasi, OD, now a Pediatric Optometry/Vision Therapy/Vision Rehabilitation resident at PUCO, feels as if she can provide more guidance to patients regarding choices affecting their overall health. She says she can see how IPC is especially important in traumatic/acquired brain injury and in pediatric cases involving developmental/learning concerns. “However, she says, “any patient with a systemic disease with multiple manifestations would benefit from IPC.” Dr. Bavasi plans to foster IPC as a practicing optometrist in a variety of ways, including providing in-service education to other healthcare professionals/specialties in her community so they are better educated about the specialized services optometrists deliver. The same goes for Sheila Morrison, OD, a fellow PUCO graduate and resident, in Cornea and Contact Lenses. Discussing her view of IPE and IPC, she says, “Right out of residency I’d like to participate as a provider in an interprofessional clinic in my community, with the intent to promote the model and potentially develop as an educator for students in the future. I believe there are varying levels of involvement, all of which are positive. Simply respecting other professions and being informed about what they do is positive, as is being an active member of an institution providing interprofessional care or education. In either case, I value IPC and will carry it forward with my career.”
